
Total Knee Replacement


What is Total Knee Replacement
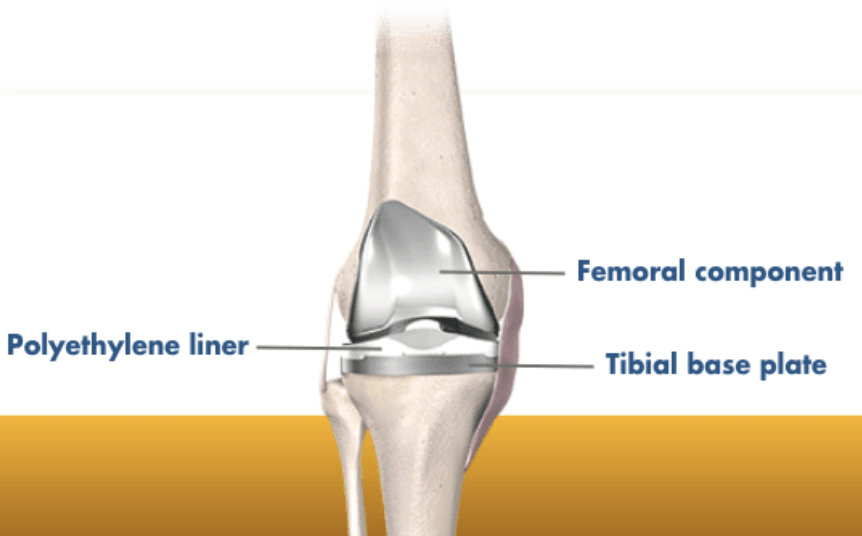
A total knee replacement (total knee arthroplasty) is a quality of life operation. It involves resurfacing the worn parts of the knee with metal (cobalt chrome and titanium) and a plastic (highly cross-linked polyethylene) spacer.
It is a highly successful operation and the replacement can be expected to last for decades (90% are still functioning after 20 years).
Who is a Candidate for a Total Knee Replacement?
Adults, usually over the age of 50, with a degenerate knee causing all or some of:
- Pain
- Stiffness
- Deformity/swelling
- Reduced mobility
These symptoms would usually have been present for many months or even years, often getting worse over time. Non-operative measures should have been tried, including weight loss, activity modification, regular analgesia, physiotherapy. Once these are no longer enough, and the knee is having a significant impact on your quality of life, then a total knee replacement can be considered.


What Does Total Knee Replacement Involve?
Once the decision has been made to proceed with surgery, Dr Ferguson will explain the procedure and the risks (see below). A date for surgery is usually planned but can be deferred. A booking form will be completed and you will be asked to sign a consent form. These forms are then taken to the Armidale Private Hospital where the administration staff will process the paperwork and check health fund details and eligibility. They will arrange for you to come to the pre-anaesthetic clinic (PAC) to see the anaesthetist and nurse, usually a couple of weeks prior to surgery.
Dr Ferguson will also give you a referral for a CT scan which you can take to i-Med Radiology (or Inverell Diagnostic Radiology) to get a scan that is used for the Mako Robotic 3D planning. This scan should be done at least 2 weeks prior to surgery.
The operation itself is usually done under a spinal anaesthetic, with a nerve block and sedation. The procedure usually takes about 60-90 mins. When you leave theatre, your leg will be wrapped in a bandage from foot to thigh (this is removed the next morning). After spending some time in recovery you will then be transferred back to your room on the ward. The physiotherapist will visit you later in the day to get you to stand and to take some steps.
As the local anaesthetic wears off, the pain will increase. You will be prescribed both long-acting and short-acting narcotic pain killers to control this. On the day after surgery, you will have a routine blood test and an x-ray. Dr Ferguson will show you the x-rays to help explain what he has done. The physiotherapist will visit twice a day to show you exercises to get your knee bending and straightening, and help with your walking. Initially, you will be walking with a frame, but usually, progress to a single walking stick by discharge.
Discharge home is usually on day 3.
Risks With Total Knee Replacement?
All operations have risks, and knee replacements are no exception. Dr Ferguson will outline these to you before you sign the consent form. They include:
- Pain
- Bleeding
- Infection
- Damage to nerves or blood vessels
- Blood clots (leg/lungs)
- Stiffness
- Fracture
- Mal-alignment
- Loosening
Apart from pain, most patients don’t have any of these problems. The risk of a complication is about 5 in 100. The risk of a serious complication, such as deep infection, is less than 1 in 100.
At home, you may notice that the knee clunks, or makes a noise when you walk or stand up. This is normal, the components are made of metal and plastic and they make a noise when they knock into each other. You will also notice that there is a patch of numbness on the front of the knee, most people have this, it is normal. The numbness is permanent but the area shrinks by 50% over 6 months.

